To improve and enhance facet fusion, expose and percutaneous methodologies to facet fusion have been characterized. The goal of this study is to explain the endoscopic component decortication with an allograft implantation approach as an adjuvant to an intramedullary union.
Endoscopic entrance to Kambin’s trapezoid, disk herniation preparedness, extensible enclosure insertion, with percutaneous implants implantation is all part of the procedure. The midline surgeon makes, and the telescope was moved to the appropriate level above the joint surfaces. After gripping forceps were used to remove the damaged tissue, cautery has been employed to rupture the aspect capsule.
Enhance fusion
Laparoscopic lumbar replacement is amongst the most recent lumbar segmentation techniques, but it has a lot of promise. The method is always changing. Full endoscopy surgery was described as reconstructive surgery through some kind of solitary incision, including continuous irrigation as well as viewing of the operational region uses a mobile phase rather than air, just like in MIS instances using tubular external rotators.
Drilling within and above the lateral aspect of the shoulder was done with an adjustable high-speed borer. Subsequently, facet fusion transplant implants were inserted into the cannula of the endoscopy.
Lumbar spinal fusion
Minimal oxygen deprivation, reduced incidence of bleeding, less disturbance of normal muscle, faster return to assistive devices, and shorter hospital stay are all advantages of a nonsurgical anterior cervical lumbar spinal fusion.
When combined with monitoring, a good facet lamination is designed to stop screw displacement. Participants who underwent dorsal or interbody merging had quite a 3.5 percent chance of being required to overcome, according to the study.
Articular coverings
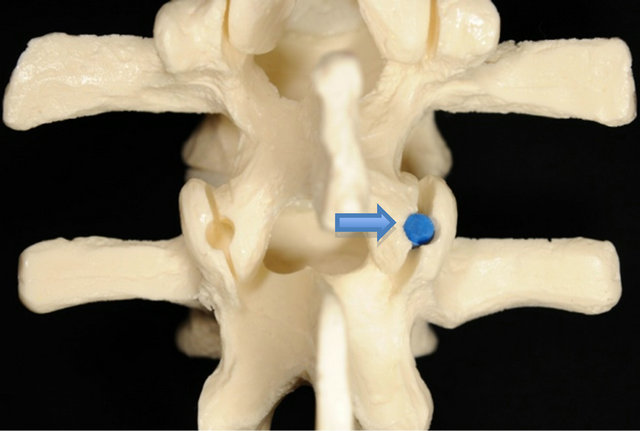
Facet joints have hyaline articular coverings and thus are vascularized by the lateral branched nerves. They are flexion and extension seen between belonging to different articular portions of two neighboring spines. Facet joints help to transmit load amongst vertebral by completely supporting axial stress concentration along with rotational and bending forces pressing on the posterior spine.
Facet fusion developed for this purpose, also known as ligamentous degenerative joint disease, is some kind of inflammatory change characterized by cell transformation, a contraction in component articular surface, and the production of osteophytes. It’s also frequently linked to pain intensity, sciatica, with neurogenic nerve entrapment.
Integrated spinal treatments
Applied load but also spine integrity is dependent on the pelvic facet. Nevertheless, it is uncertain if the integrated surgical treatments are appropriate including all individuals with component joint arthropathy, independent of the complexity of their condition before surgery.
The goal of this longitudinal analysis was to see how the degree of pretreatment facet articulation arthropathy affected functional results as well as spinopelvic orientation in participants who had lumbar-stability maintaining decompression with Dynesys implantation. The expected outcomes might assist to explain the surgical justification for ligamentous displacement with stabilization.
Minimize neighboring segment
To minimize neighboring segment deterioration, the posterior cervical muscle was separated symmetrically out from joint surfaces inside this subperiosteal level, and also the backside tension zone in the sacred duty tendons was retained at some of the most lateral aspects ligamentous levels.
Following the removal of the facet fusion, the afflicted segments underwent lumbar security displacement with complete bilateral surgical intervention but also facetectomy, as reported previously.
For appropriate relaxation in children with chronic stenosis, the complete facetectomy from less about 25% was done symmetrically.
Aspect of connections
Its independent – sample t and chung analysis were used to evaluate demographic characteristics as well as pretreatment clinical features across subgroups. All clinical features of each intensity group were then compared both during surgery using a within-group assessment. Furthermore, a blended model univariate analysis was used to examine the variations in clinical features between categories sometimes during operation.